
IOL Services - Contrast Sensitivity
Background
Whilst many patients retain good visual acuity when developing a cataract, they may experience a loss of other visual functions such as contrast sensitivity (CS).1 CS can be defined as the ability to detect luminance contrast and is usually described as the reciprocal of the minimum perceptible contrast.2
Uses
CS assessments are useful for identifying the full extent of visual function loss, so as to evaluate the need for prompt cataract surgery. They are also used for evaluating differences in CS with aspheric versus spherical intraocular lens (IOL) designs,3 and for measuring losses in CS with multifocal designs.4
Conventional Tests
Common CS tests include the Pelli Robson chart, the Functional Acuity Contrast Test (FACT) and the CSV-1000 instrument. Figure 1 highlights the relevant parts of the CS function evaluated by each instrument. Each of these tests has some disadvantages; e.g. the Pelli Robson chart only evaluates CS at one spatial frequency, whereas the FACT test and CSV-1000 device use a limited 'forced-choice' scoring, which is liable to 'guessing' errors leading to 'ceiling' and 'floor' effects.5
Our Approach
An 'ideal' CS test should measure a number of different contrast levels over a range of spatial frequencies as shown by the yellow line in Figure 1. CS measurements under mesopic and photopic conditions, both with and without a glare source, may also prove useful to better predict visual performance under different illumination conditions and over a range of pupil sizes.
A better understanding of visual performance with modern IOLs is helpful in providing optimal IOL solutions for cataract patients.
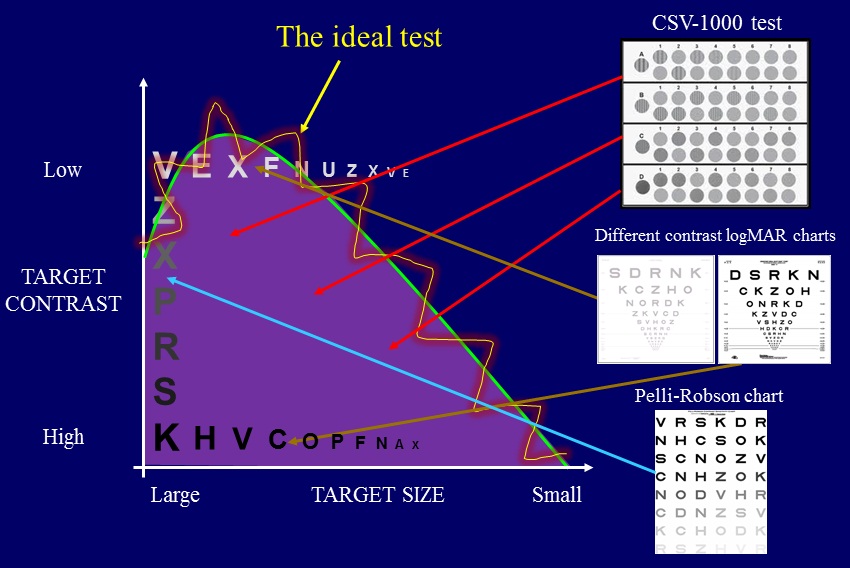
Figure 1. The contrast sensitivity function (CSF) curve demonstrating areas of the CSF assessed by different tests methods. The 'ideal' test would display optotypes at several levels of contrast over a wide range of spatial frequencies (yellow line).
References
- Elliott DB & Situ P. Visual acuity versus letter contrast sensitivity in early cataract. Vision Res. 1998;38: 2047-2052.
- Owsley C. Contrast sensitivity. Ophthalmology Clinics of North America. 2003; 16:171-177.
- Montes-Mico R, Alio JL, Munoz G & Charman WN. Temporal changes in optical quality of air-tear film interface at anterior cornea after blink. Invest Ophthalmol Vis Sci. 2004; 45:1752-1757.
- Leyland M & Pringle E. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2006: CD003169.
- Pesudovs K, Hazel CA, Doran RM & Elliott DB. The usefulness of Vistech and FACT contrast sensitivity charts for cataract and refractive surgery outcomes research. Br J Ophthalmol. 2004; 88:11-16.